

If your answer is YES, you may have osteo-arthritis of the hip joint also called hip OA.
Unlike back pain or sciatica, hip OA pain is usually felt in the groin and sometimes radiates into the thigh as far down as the knee. Stiffness of the hip joint is another common symptom. With advanced OA patients struggle to weight bear, require crutches and are sometimes unable to run their own household and are unable to work.
The hip joint is one of the largest joints in the body. It is a spherical ball and socket joint made up of the femoral head (ball) and the acetabulum (socket). The ball and socket is lined with very smooth hyaline cartilage. It is wear and tear of this cartilage that leads to the development of OA. The cartilage wear can be initiated by excessive use or injury at work or sport and or overloading due to obesity. Familial predisposition to OA also plays an important role.
The initial treatment of hip OA includes regular simple painkillers and anti-inflammatory medication as tolerated, soft well-cushioned walking shoes, a walking stick and physio or hydrotherapy.
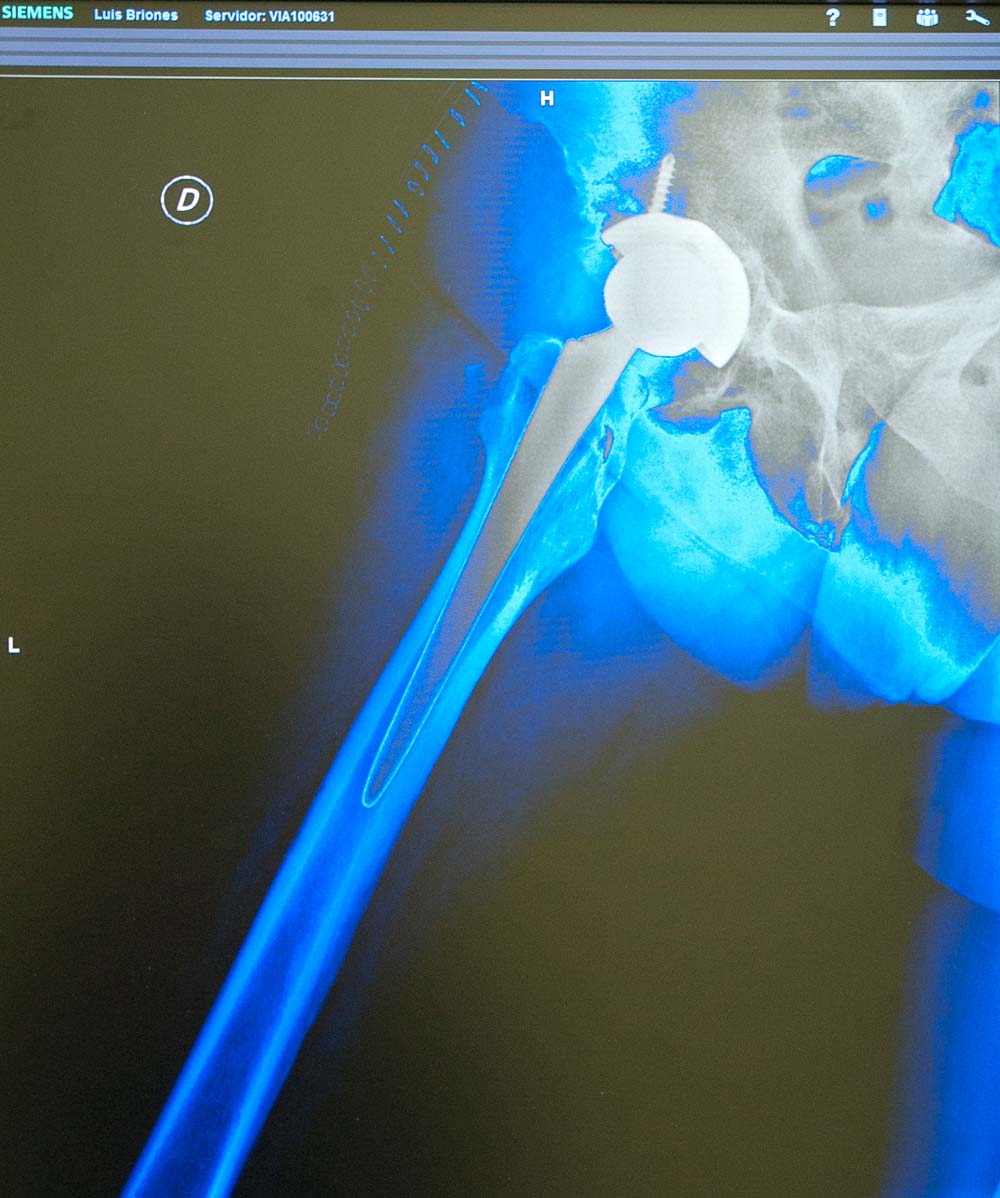
When OA hip pain can no longer be managed with painkillers etc. hip replacement surgery should be considered. A simple hip x-ray will confirm the diagnosis of hip OA.
Most patients undergoing hip replacement are in their 6 or 7 decade. Some are younger and some much older. The decision to have a hip replacement should be based on the severity of symptoms and associated loss of function. X-rays help the surgeon to understand the disease progress but are not an indication for surgery.
Hip replacement implants are made up of an acetabular component that is fitted into the hip socket and a femoral component that is introduced into the upper thighbone.
Depending on the patients bone quality and surgeon’s preferences the implants can be introduced press-fit without cement or alternatively fixed with bone cement.
The joint bearing itself is attached to these components. Modern hip replacement bearings are made of a combination of metal-on-highly-cross-linked polyethylene, ceramic-on-polyethylene or ceramic-on-ceramic. Metal-on-metal bearings became again popular in the early 2000’ with so-called hip resurfacing procedures. However unacceptably high failure rates of the metal-on-metal bearing, significant acetabular bone loss and other health concerns have led to the decline of their use.
This includes obtaining a detailed history and examination by the orthopaedic surgeon. The surgeon will template the chosen hip implant for size and position using a digital x-ray image and a special templating software. This helps to recreate correct leg length, correct centre of rotation and correct femoral offset.
If there are any known health problems the opinion of a physician or cardiologist is sought. All patients have preoperative blood tests, ECG, multiple microbiological swabs, urine analysis and x-rays. Surgery will only take place if all results are acceptable.
Prior to surgery the anesthetist will discuss the preferred type of anaesthetic and the post-operative pain management plan.
Patients also meet Eva Rando, the senior Physiotherapist, prior to surgery to learn the use of crutches and the do’s and do not’s of hip replacement.
During the surgery the patient is positioned lying on the side. The pelvis held firmly by positioning devices. The hip and leg are disinfected and draped. The surgeon will open the hip from the side. First the femoral head is taken out of the socket and removed. The acetabulum is then prepared and sized to accept the acetabular component, which is usually press fit. The attention is the turned to the thighbone. This is opened and broached to receive the femoral component. A trial reduction with a temporary femoral component and head is carried out to check the joint geometry before the definitive implants are inserted. The hip can then be closed. Surgery times vary but are usually well below one hour. After surgery the patient is taken to the recovery area for direct one-to-one observations before returning to their room.
Most patients can get up with supervision and take some steps a few hours after surgery. All patients will have physiotherapy by the next morning. The arthritic hip pain will be gone after surgery. There will however be pain related to surgery. Multimodal pain relief is provided by the initial spinal anaethetic, an optional fascia iliaca block, patient controlled analgesia and prescribed painkillers. Patients also receive injections to minimize the risk of venous blood clots.
Older patients often choose to stay longer to take advantage of regular physiotherapy and nursing care until they feel comfortable and safe to return to their own home.
Patients will be reviewed by the orthopaedic team every day whilst at HC Marbella Hospital Internacional and by Dr. Boerger at 2 weeks for wound review, at 6 weeks, 6 months and one year with new x-rays. For patients travelling from abroad 6 week to one-year follow-ups can be scheduled at their place of residence.
Activities that must be avoided after after total hip replacement include crossing legs whilst sitting, low chairs or toilets (a raised toilet seat is recommended), lying on the side, bending to the floor to pick up items or putting on shoes, cutting your toenails etc.
Once at home it is ideal to keep all items of daily living at a convenient height, have a helper for household chores and perhaps some prepared meals in the fridge or freezer.
Loose carpets and rugs should be removed to reduce the risk of tripping and falling. Anti-slip mats should be used in the bathroom and shower. Using the bathtub should be altogether avoided for 6-10 weeks.
Most patients will use one or two crutches for about 6 weeks. Mobility rapidly improves and normalises by 3-6 months.
Patients can drive a car when mobile without crutches.
However there are risks and potential complications. These can be divided into:
– Common risks: pain, bruising, bleeding, leg length discrepancy.
– Less common risks: deep vein thrombosis, infection, fracture of bone, implant mal-position, dislocation of hip.
– Rare risks: pulmonary embolism, stroke, cardio-vascular collapse and death.
A hip replacement can wear out or become loose with time. This sometimes requires re-do or revision operation. Last generation implants are expected to last well in excess of 10 years, often much longer. The UK, Australian and Swedish National Joint Registries are a very good source of information on hip implant survival times for different types and makes of hip replacements.
High-impact activities, such as regular running or field games must be avoided. Low impact activities such as swimming, rowing, sailing, golf, hiking, riding a bike and gentle doubles tennis are well tolerated with a total hip replacement.
Dr. Thomas Boerger MD FRCSI (T&O), Orthopedic and Trauma Surgeon performs primary hip and knee replacement surgery, revision surgery of the knee and arthroscopic surgery of the knee.
In 2017 Dr. Boerger performed over 300 procedures with just under 150 joint replacement operations.
His recent joint replacement audit for 2017 confirmed no infections and a very low rate of complications.
Traumatology and Orthopaedics Specialist.
June 21, 2018
Read other news
Tel.: +34 952 908 628
+34 609 148 799
952908898 Oncology
951829978 Diagnosis by imaging
951829947 Gynecology
952908897 Fertility
951829947 Physiotherapy



