

Cancer treatment is continuously evolving achieving significant advances in cure rates and increasing patient survival.

Tumours are formed from normal tissue cells and produced through changes in their DNA called “mutations”. When there is a mutation, the cell changes completely and starts to divide uncontrollably, developing into cancer
Until a relatively short time ago these tumours were classified according to the tissue of origin: lung cancer, breast cancer, liver cancer… and from there the patient was sent to the lung specialist, breast specialist, liver specialist… But the site of origin does not define the tumour, or at least it only defines it in part. For the first time we have the capacity to sequence (analyse) the DNA (genome) of each tumour. This allows us to understand what is happening based on an existing mutation. And we can design “a la carte” drugs, known as specific targeted agents, which target one or more specific mutations.
Many of the usual cancer treatments: surgery, radiotherapy and also chemotherapy, can be curative as they are constantly evolving and achieving better therapeutic results. Mortality due to cancer is reducing at a rate of 2% a year and constantly increasing quality of life for the patient.
As a result cancer surgery is becoming continually less aggressive and less mutilating. Successful preservation of the organ in which the tumour develops is possible on many occasions now that other supplementary treatment is given (radiotherapy and chemotherapy) with surgery being performed afterwards using more efficient and safer techniques.
Radiotherapy has also developed significantly, often being as effective as surgery thanks to new sophisticated radiotherapy machines which achieve selective destruction of the tumour with little effect on the surrounding tissue.
 Chemotherapy is the third therapeutic weapon against cancer and is known, together with hormone therapy, as systemic treatment as it is given to the patient either parenterally or orally. Chemotherapy has also developed significantly. These systemic treatments are increasingly used earlier, in conjunction with surgery and with radiotherapy before and afterwards, as a means of preventing possible recurrence later on. Chemotherapy has also achieved control, sometimes definitively, as a single therapeutic weapon in tumour processes even at an advanced stage, as well as in leukaemia, lymphoma, some childhood tumours, testicular cancers, etc.
Chemotherapy is the third therapeutic weapon against cancer and is known, together with hormone therapy, as systemic treatment as it is given to the patient either parenterally or orally. Chemotherapy has also developed significantly. These systemic treatments are increasingly used earlier, in conjunction with surgery and with radiotherapy before and afterwards, as a means of preventing possible recurrence later on. Chemotherapy has also achieved control, sometimes definitively, as a single therapeutic weapon in tumour processes even at an advanced stage, as well as in leukaemia, lymphoma, some childhood tumours, testicular cancers, etc.
All this has been due to the development of more and more new agents specifically targeted at different mutations identified in the tumour. This last group of agents consists of those known as “Targeted Therapy” (drugs which interfere with specific mutations which cause cancer) they currently play an important role and represent a significant step forward, leaving behind the classic concept that the same treatment works for all tumours.
But one of the most important therapeutic advances, currently and for the future, is the immunological treatment of cancer, known as immunotherapy. This incorporates highly effective agents achieving control of some advanced tumours which were previously uncontrollable, even being curative in some cases. These treatments are different to previously due to a different mechanism of action.
The immune system is one of the most efficient systems in the body and usually exists as a physiological defence against any type of attack on it. This system has evolved over thousands and thousands of years and is devoted to defending against the actions of external agents, allowing human beings to survive in a hostile environment.
It is made up of a large variety of cells with specific functions which act in a coordinated manner to recognise and eliminate abnormal cells from the body. These abnormal cells have on their surface, or release when destroyed, molecules called antigens which stimulate the immune system to produce a response using antibodies.
One significant component in this response is the activation and production of T lymphocytes which function to neutralise or eliminate these abnormal cells. These T lymphocytes are activated by the presentation of the previously described antigens by special cells from the immune system called Dendritic Cells, their main role being to present activation antigens.
Activated T lymphocytes are those which act on the tumour cells and cause their destruction. Image 1.
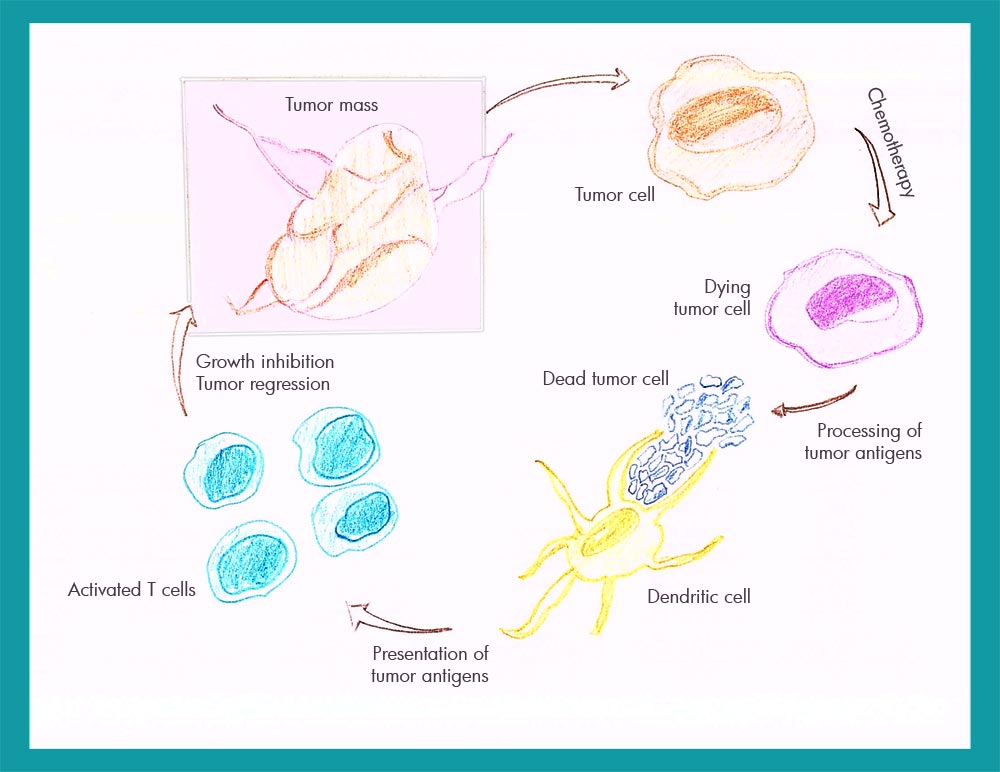
The problem which occurs with malignant tumours is that at a determined time, still not fully understood, the destructive action of these lymphocytes is neutralised or reduced due to the action of factors produced by the tumour. Sometimes this neutralisation is not complete and the patient’s immune system works weakly, the tumour then grows more slowly although finally succeeds in spreading and killing the patient.
These concepts which have been understood for a long time have resulted in the development of drugs targeted in unblocking the system which paralyses the destructive action of the lymphocytes. It is the basis of current immunotherapy which we will try to explain in the simplest way possible.
To be able to perform this “unblocking” action a series of agents, monoclonal antibodies, have been developed which work in patients to recover their defensive capabilities. A new therapeutic era has been founded through the use of what are known as Immunotherapy Agents.
The first to benefit from this new era are patients who suffer from more aggressive tumours with little possibility of obtaining any response with conventional treatment. This is the case with malignant melanoma, a skin tumour which takes thousands of lives a year throughout the world and which has been the first to rely on this immunotherapy, demonstrating a high level of success with a significant increase in survival.
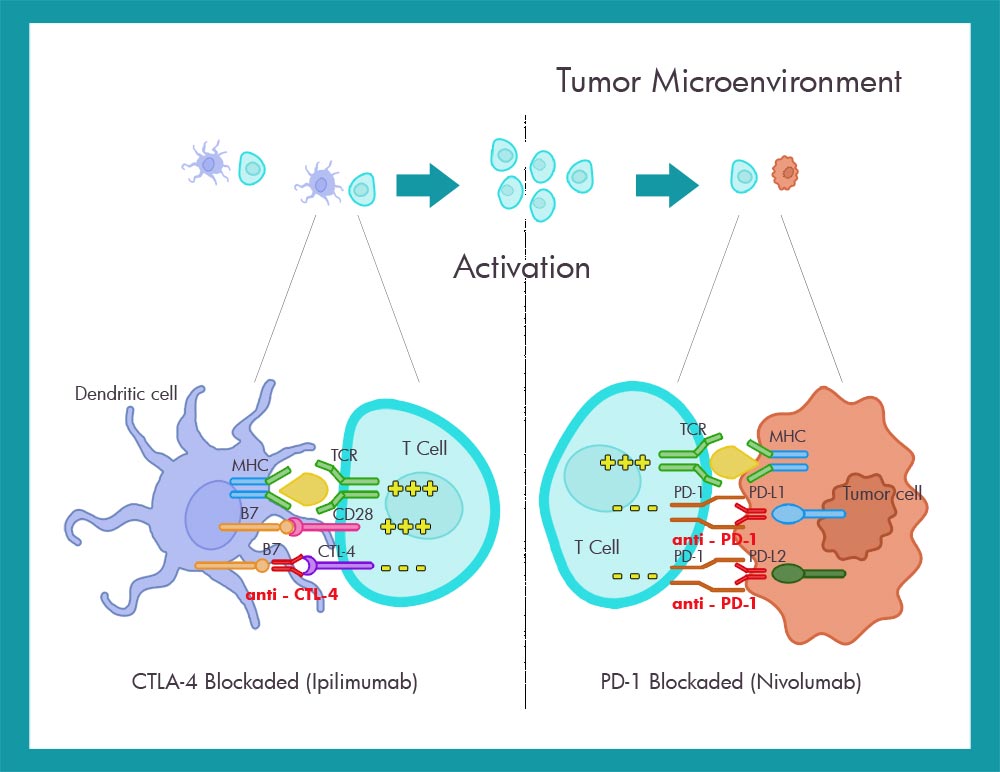
The drugs are Monoclonal Antibodies (mAb) which act at the level of lymphocyte receptors and tumour cells, freeing the inhibition that the tumour causes and allowing them to act as destructive elements at the level of the interference points. Due to action on these points they are known as Checkpoint Inhibitors.
The first of this type of drug was developed by BMS (Bristol Meyers Squib) and was called Ipilimumab which blocks the inhibiting action of a T Lymphocyte receptor, called CTLA 4. This receptor hampers the T cell’s action, blocking it allows the T cell to recover its destructive action (Anti CTLA 4).
Ipilimumab was tried out as a single agent in advanced melanoma more than 4 years ago achieving a high response rate which prompted the rolling out of a broad development and clinical research programme.
The second drug investigated by the same company BMS was Nivolumab which acted on another T Lymphocyte receptor called PD1 that under normal conditions would act on the tumour cell through some ligands known as PDL1 and PDL2, but they were neutralised by the tumour preventing them from having their destructive effect (anti PD1).
Image 2
Both agents (Ipilimumab and Nivolumab) have been used as single agent treatments and in combination.
They have achieved a response rate greater than 60% with complete remission in 22% of patients with very advanced metastatic melanoma.
 Given these responses in melanoma, research into other tumours such as advanced lung cancer with poor prognosis, pancreatic cancer, liver and colorectal tumours and tumours of the head and neck has been carried out.
Given these responses in melanoma, research into other tumours such as advanced lung cancer with poor prognosis, pancreatic cancer, liver and colorectal tumours and tumours of the head and neck has been carried out.
Simultaneously other laboratories have developed similar agents such as Pembrolizumab (AntiPD1) from MSD for melanoma and renal carcinoma and Atezolizumab (Anti PDL1) from Roche for lung cancer and also urothelial tumours.
The magazine «Nature Reviews Clinical Oncology» recently published a review of more than 200 scientific articles carried out by the National Oncological Investigation Centre (Centro Nacional de Investigaciones Oncológicas – CNIO) which revealed the future potential for immunotherapy to improve survival in pancreatic cancer.
As a result the team led by José Antonio López Martin, Head of the Oncology Early Phase Clinical Trials Unit (Unidad de Ensayos Clínicos en Fase Temprana en Oncología – UFTO) in the 12 de Octubre University Hospital, indicated that “we find ourselves on a ‘changed course’ thanks to the appearance of new treatments designed to activate the immune system so it recognises and directly attacks the tumour”.
Due to this we believe that it will be necessary to establish individual criteria for this type of molecule, given the results which we are seeing.” It is also a challenge for the pharmaceutical laboratories.
Video about Immunotherapy
In the Oncology Unit in our HC Hospital we have already been giving Immunotherapy treatment for a couple of years, generally with excellent results.
We started to use Ipilimumab (Anti CTLA4) in advanced melanoma and currently we are using Nivolumab and Pembrolizumab (Anti PD1) also in melanoma and in advanced lung cancer. This has been possible thanks to the Expanded Access Programme from Bristol Myers Squib and Merck Sharp & Done (MSD) Laboratories.
The results obtained up until now are equivalent to those reported in the literature with very high response rates and excellent treatment tolerance.
Some of these drugs are already available with limited indications having been approved by the European and Spanish Agencies and we are hoping that both insurers and the National Health System will cover their high cost.
Director of Oncology Service of HC Marbella
March 1, 2016
Read other news
Tel.: +34 952 908 628
+34 609 148 799
952908898 Oncology
951829978 Diagnosis by imaging
951829947 Gynecology
952908897 Fertility
951829947 Physiotherapy



