Dr. Nuño Cristina
Radiotherapy Oncology Specialist

Radiotherapy uses ionising radiation in the area to be treated, with the aim of destroying cancer cells and preventing them from reproducing.
Due to technological advances over recent years, radiotherapy is currently safe, painless and effective, and delivers very good results. In the majority of cases patients can continue with their normal daily lives during treatment.
It is a fundamental part of multidisciplinary cancer management, with the capacity to destroy cancer cells and prevent their growth and reproduction.
Radiotherapy is a local treatment, therefore only affecting the part of the body which is targeted.
Both the preparation and application of treatment require very complex technology. This technology has advanced greatly in the last few decades allowing more precise and safe radiotherapy treatment to be offered, greatly reducing possible side effects.
A linear accelerator generates a high amount of energy (electrons). These electrons are accelerated, colliding with a target, causing high energy X-rays. These X-rays target the treatment zone, damaging DNA and causing cell death in the tumour cells, preventing their reproduction and spread. During this process, the patient cannot see, smell or feel the radiotherapy, as we often say, “you just have to believe”.
Neither do patients go home with radiation in their body, allowing them to continue to be with children or pregnant women following treatment.
Radiotherapy is generally well tolerated and is given on an outpatient basis. Although treatment requires several sessions, the latest technological advances have meant treatments are becoming shorter and shorter, whilst still being equally effective.
Ionising radiation causes breaks in the DNA molecules, damaging their function, encouraging cell death and destroying their capacity to reproduce.
Cancer cells are slightly more sensitive to radiation than healthy cells.
Treatments are programmed with submillimetre precision, with the aim of affecting the tumour cells whilst reducing the dose to healthy tissue as much as possible.
70% of oncology patients will require radiotherapy.
Radiotherapy treats cancer at its source and the aim varies depending on when it is given.
Radiotherapy treats cancer at its source and the aim varies depending on when it is given.
The duration of treatment from when the patient enters the machine until they leave usually lasts around 20-25 minutes. This period of time includes:
In other words, the irradiation itself only lasts around 2-5 minutes. There are patients whose positioning may take more time due to their physical condition, or due to tumours which have undergone changes during treatment, making verification more complex.
Treatment is always individualised, in other words, each patient has their own specific treatment, which differs to any other patient.
Giving ionising radiation for therapeutic reasons requires a laborious technical and clinical process.
Following the first consultation with the radiotherapy oncologist, where treatment is explained to the patient, preparation for radiotherapy treatment begins and involves several phases:
Simulation:
Firstly, we determine which is most appropriate position for treatment.
Once the position has been defined, we use different moulds, or casts, to immobilise the patient, the lasers are aligned, the exact positioning coordinates are recorded and the skin is marked. This enables us to reproduce the exact same position during treatment sessions.
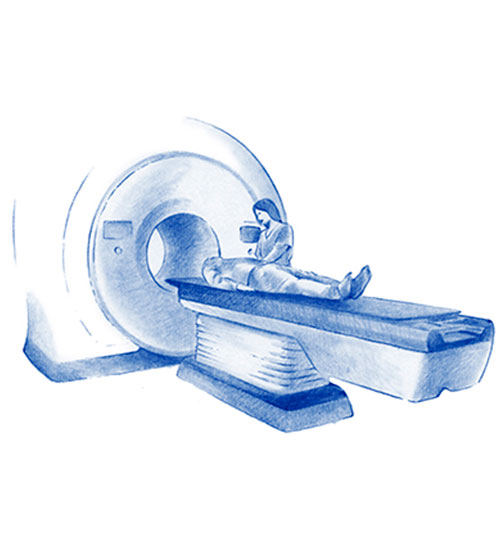
We obtain an image with a CT planning scan that allows the radiotherapy oncologist to locate and determine the area to be irradiated, as well as the healthy tissue in the area which must be protected from radiation. Simulation can be done with PET-CT or with CT alone depending on the location and type of tumour.

Planning:
Planning consists of determining the dose of radiation and the method for its administration.
Selection of the best treatment plan for each patient is assessed jointly by the radiotherapy oncologist and the radiophysicists.
The radiotherapy oncologist defines the treatment volume and determines the dose which must be reached in that volume. The adjacent healthy structures are also defined to protect them and ensure that they receive the minimum dose possible, always a dose that they can tolerate well.
The radiophysicist, is responsible for distributing the dose prescribed by the doctor, in other words, precisely determining the features of the radiation beam for that specific treatment, in compliance with the requirements established by the radiotherapy oncologist.
Application and verification of treatment:
The aim is to verify that simulation and planning are correct.
An imaging test is required for correct verification to ensure correct administration of treatment. CT enables us to see the tumour, or area to be treated, at that moment in time, ensuring that there has been no change and that the dose is targeted exactly at the area.
This is done in the machine where treatment is going to be given, so that the patient does not need to move, but simply needs to remain still in the machine in the established position.
The doctor, together with the technicians, verifies that the treatment parameters are correct and that there are no new changes on imaging, then giving the go ahead for treatment to be given.

Depending on the aim of treatment (curative/palliative) the expected response will be at a clinical, symptomatic level, or at a radiological level. As radiotherapy causes changes in cells, it does not have an immediate effect, on occasion a reduction in size or changes in tumour can continue to be seen even months after treatment.
When we want to achieve symptomatic relief, then we see the response as pain relief, cessation of bleeding or recovery of function.
However, when the intention is to eradicate or control disease, an initial imaging study (CT, MRI or PET-CT) is indicated at 2-3 months after finishing treatment, to compare the size and activity of the tumour in relation to tests prior to treatment. Following on, monitoring is then performed following an initial period of 3-6 months to check response to treatment. An imaging study is not indicated as soon as treatment finishes as oedema/inflammation will probably be seen and/or a lack of response. There are times when a response is seen during treatment, a reduction in tumour size may be seen on the daily image monitoring prior to each session.
Throughout our lives we are exposed to many types of radiation. For the most part it is environmental, coming from natural sources such as the earth on which we live, the sun, the air we breathe, the water and the food we consume.
The whole radiotherapy department relies on special radiological protection measures which ensure that the radiation dose absorbed by our centre’s personnel is at a minimum.
The staff who have most contact with the radiotherapy department are obliged to carry a dosimeter which guarantees that the dose of radiation absorbed is not dangerous and is within established limits.
The accelerator only emits radiation when it is in use. Once the patient leaves the machine they are not left with any radiation in their body and can therefore continue to be with children and pregnant women without any risk.
The accelerator is within a bunker with concrete walls which are 1.5 m thick and comply with very strict technical specifications, as indicated by the Nuclear Safety Council. The council verifies the installation and gives the go ahead and authorisation on behalf of the Ministry for the Ecological Transition.
Within the Radiotherapy Department there is a Quality Assurance Committee, responsible for developing an assurance plan, to comply and inform the competent authorities of any error.
The radiophysicist continually checks that the condition of the machine is optimal and that there is no risk.
Our accelerator is also monitored by its manufacturer in Madison, USA.
Dr. Nuño Cristina
Radiotherapy Oncology Specialist

Dr. Trigo, José Manuel
Director of Oncology, Research and Innovation
Dr. Cortés-Funes, Hernán
HC Marbella Presindent
Specialist in Medical Oncology

Dr. Jiménez Rodríguez, Begoña
Specialist in Medical Oncology
Clinical Dedication in Breast and Gynecological Cancer

Dr. Villatoro Roldán, Rosa Mª
Specialist in Medical Oncology

Dr. Llácer Pérez, Casilda
Specialist in Medical Oncology
Clinical Dedication in Digestive Tumors and Colon Cancer

Dr. Sedano Ferreras, Paula
Radiotherapy Oncology Specialist

Dr. García Baltar, José Antonio
Especialista en Radiofísica Hospitalaria

Dr. Ponce Aix, Santiago
Medical Oncology Specialist
Clinical Dedication in Lung Cancer
Precision medicine
Cancer immunotherapy

Dr. Bennis, Mohamed Hassan
Oncology Specialist
Clinical Dedication in Lymphomas

Tel.: +34 952 908 628
+34 609 148 799
952908898 Oncology
951829978 Diagnosis by imaging
951829947 Gynecology
952908897 Fertility
951829947 Physiotherapy