Dr. Gismero Moreno, Saturnino
Jefe de servicio
Oftalmólogo especialista en Retina

People with diabetes are 25 times more likely to suffer blindness than the rest of the population. Fortunately, proper control of the disease and timely therapeutic action have proven to be effective in preventing this from occurring.
This requires the patient to be aware of his or her condition, to have a medical follow-up by a diabetes specialist, to visit the ophthalmologist regularly and to maintain a disciplined and healthy lifestyle in terms of diet, physical exercise, weight, etc. This way, an early diagnosis can be achieved and preventive action can be taken.
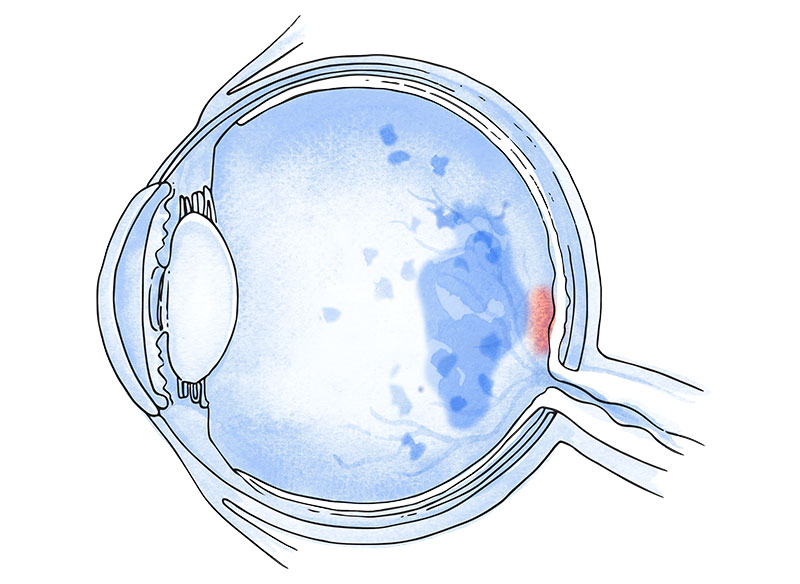
Just as the metabolic decompensation caused by diabetes affects other organs, chronic hyperglycaemia also damages the blood vessels of the retina. Diabetic retinopathy and diabetic macular oedema are the main secondary pathologies of diabetes involving retinal damage.
In the case of the former, the alteration of macular microcirculation can lead to a decrease in the supply of oxygen to the retina, preventing it from receiving the necessary amount for its proper functioning. This condition is known as ischaemia and can lead to the death of neuroretinal neurons. As nerve tissue does not regenerate, the damage caused is irreversible.
A “waterlogging” of the macula can also occur due to the alteration of the blood vessels of the macula and/or the inflammatory nature of the disease, which can lead to the leakage of intravascular fluids, causing macular oedema. This requires appropriate treatment to prevent loss of vision.
Diabetic retinopathy can have other detrimental effects on vision:
- Diabetic vitreous haemorrhage: new blood vessels appearing after ischaemia tend to bleed more easily, which tints the vitreous humour, compromising its transparency and leading to consequent loss of vision.
- Tractional retinal detachment: The vitreous gel contracts when invaded by neovessels. This can displace the retina to the point of separating it from the wall of the eyeball and/or rupturing it.
- Tractional macular oedema: Other times traction occurs gently on the macula, producing a different oedema to the one mentioned above (tractional versus vasogenic/inflammatory), as its origin is different. This oedema is not related to vascular deterioration or to the inflammatory nature of diabetes.
The main one is the time of evolution of diabetes, as well as not achieving good metabolic control. It is vital that diabetic patients undergo a complete ophthalmological check-up at least once a year, since poor metabolic control favours retinal lesions.
In addition to measuring blood glucose levels by means of a finger-prick test, the percentage of glycosylated haemoglobin should also be studied periodically. This will help us to identify any undetected hyperglycaemia.
There is scientific evidence that if the glycosylated haemoglobin is less than 6.9%, the incidence of diabetic retinopathy and diabetic macular oedema is reduced. However, it is also very important to avoid hypoglycaemias, which have been proven to be very harmful.
The ophthalmologist will perform an examination of the fundus including:
The treatment of diabetic retinopathy and diabetic macular oedema requires a high degree of specialisation and state-of-the-art technology.
The aim of treatment will be to control the disease and slow its progression. However, it is important to remember that the best approach is the preventive one, that is, keeping diabetes, blood pressure and cholesterol levels under control, as well as following healthy lifestyles.
Laser treatment
Called focal treatment when it is for oedema, and panretinal photocoagulation when it is used to treat diabetic retinopathy. Argon laser treatment is very effective for advanced diabetic retinopathy, as it prevents blindness. It is an outpatient treatment performed in the doctor’s office. It can cause discomfort, reduce the field of vision and worsen night vision, but it is usually well tolerated by most patients. It requires 3 to 4 sessions for each eye.
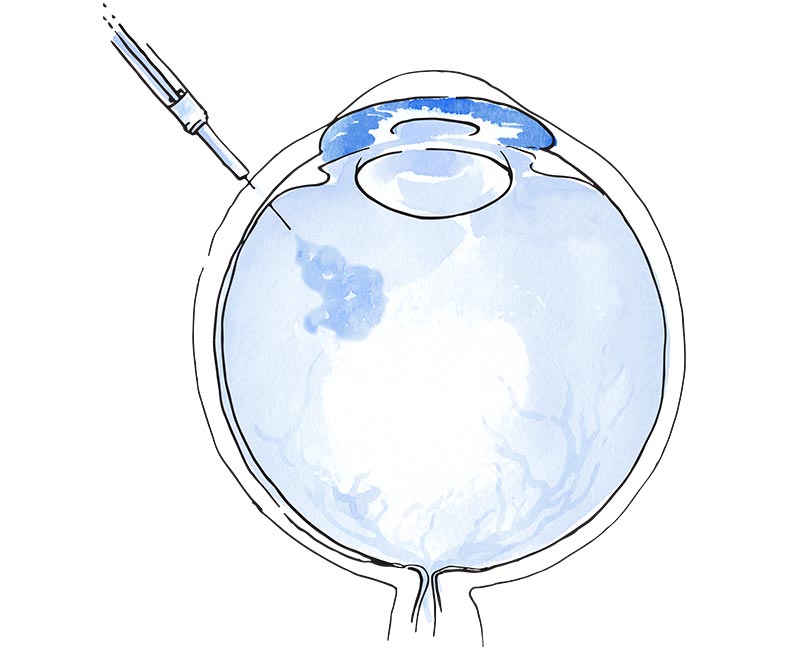
Anti-VEGF drugs
Another option to treat diabetic retinopathy is the use of intraocular injections, which can also avoid many of the adverse effects of laser treatment. However, the effect is transient so it is essential that the injections, which must be administered regularly, are not interrupted. If this were to happen without supervision, the prognosis can seriously worsen. It is very important that they are supervised by an ophthalmologist with expertise in diabetes.
Treatment for diabetic macular oedema
Even when retinopathy is not at an advanced stage, diabetic macular oedema can cause significant vision loss. This condition is currently treated with:
Dr. Gismero Moreno, Saturnino
Jefe de servicio
Oftalmólogo especialista en Retina

Dr. Alberte González, Antonio
Oftalmólogo
Especialista en Glaucoma
Dr. Flores Márquez, Ana
Oftalmóloga especialista en retina médica

Dr. Álvarez López, Alejandro
Cirugía oculoplástica y orbitaria

Partal, Carlos
Óptico y optometrista clínico
Tel.: +34 952 908 628
+34 609 148 799
952908898 Oncology
951829978 Diagnosis by imaging
951829947 Gynecology
952908897 Fertility
951829947 Physiotherapy